A patient presents with fever, cough, SOB, and a recent history of COVID-19. A PCR test was positive for COVID-19. The provider documents a final diagnosis of “pneumonia with history of COVID-19.”
What ICD-10-CM coding is reported?
The gastroenterologist performs a simple excision of three external hemorrhoids and one internal hemorrhoid, each lying along the left lateral column. The operative report indicates that the internal hemorrhoid is not prolapsed and is outside of the anal canal.
What CPT® and ICD-10CM codes are reported?
(The documentation states: “A punch is placed and pushed downward to obtain a tissue sample for a biopsy of thelunula.” What anatomical structure is being biopsied?)
A patient undergoes CABG using the right internal mammary artery anastomosed to three coronary arteries.
What CPT® coding is reported?
A 78-year-old patient experiencing intermittent asthma with exacerbation is in her pulmonologist ' s office for a pulmonary function test. The pulmonologist tests for spirometry, vital capacity,
breathing capacity, and flow volume capturing the measurements before and after administering a bronchodilator.
What CPT® and ICD-10-CM codes are reported?
A patient with jaundice was seen by the physician to obtain liver biopsies. A needle biopsy was taken using CT guidance for needle placement. The physician obtained two core biopsies, which
were then sent to pathology. What CPT® codes are reported?
A 67-year-old male presents with DJD and spondylolisthesis at L4-L5 The patient is placed prone on the operating table and, after induction of general anesthesia, the lower back is sterilely prepped and draped. One incision was made over L1-L5. This was confirmed with a probe under fluoroscopy. Laminectomies are done at vertebral segments L4 and L5 with facetectomies to relieve pressure to the nerve roots. Allograft was packed in the gutters from L1-L5 for a posterior arthrodesis. Pedicle screws were placed at L2, L3, and L4. The construct was copiously irrigated and muscle; fascia and skin were closed in layers.
Select the procedure codes for this scenario.
A woman with vulvar intraepithelial neoplasia (VIN II) undergoes a partial vulvectomy ( < 80%) with removal of skin and deep subcutaneous tissue.
What CPT® and ICD-10-CM codes are reported?
A 47-year-old male recently injured as a passenger in a car accident sustained multiple fractures. The patient now has physical restraints due to pulling out foley catheter, IV catheters and
attempted to pull out NG tube. Emergency department physician is asked to come see patient and injects 0.5 lidocaine into lumbar region of the spine. An indwelling catheter is placed into the
lumbar region for continuous infusion with fluoroscopy for pain management.
What CPT® is reported for the Emergency department physician?
911 is called by the physician for an ambulance with non-emergency basic life support to pick up a patient from his office that had fainted. The patient was taken to the hospital. What HCPCS
Level II coding is reported for the ambulance ' s service?
(A 60-year-old man presents for examination of the entire rectum andsigmoid colon. Two polyps are found in the sigmoid colon and removed usingablation. What CPT® and ICD-10-CM codes are reported?)
(Patient with erectile dysfunction is presenting for a penile implant. Anon-inflatable penile prosthesisis inserted. What CPT® code is reported for this service?)
(Procedure date:01/12/20XX
Surgeon:MD |Assistant:PA
Preoperative diagnosis:Dry gangrene of the left foot in the setting of peripheral vascular disease. Non-pressure chronic ulcer on toe.
Postoperative diagnosis:Dry gangrene of the left foot in the setting of peripheral vascular disease. Non-pressure chronic ulcer on toe.
Procedure:Amputation at the metatarsophalangeal joint of the left third toe
Indication:63-year-old female with peripheral vascular disease; vascular workup determined no further interventions to improve vascularity; third toe became progressively dusky; wound formed distally with chronic ulcer; amputation necessary; risks/benefits discussed.
Description:Left foot and third toe marked; 1 g Ancef given; general anesthesia; supine; calf tourniquet; timeout; tourniquet inflated (no Esmarch); total tourniquet time 5 minutes; tennis racquet incision with longitudinal arm over third metatarsal encircling joint proximal to closure; extensor/flexor tendons and collateral ligaments excised sharply; toe removed; tourniquet released; superficial bleeders cauterized; washed out; skin closed with 3-0 nylon; dry dressing; to PACU in good condition; signed 01/19/20XX 09:41.
Question:What CPT® and ICD-10-CM coding is reported?)
A patient who has colon adenocarcinoma undergoes an open partial colectomy. The surgeon removes the proximal colon and terminal ileum and reconnects the cut ends of the distal ileum and
remaining colon.
What procedure and diagnosis codes are reported?
A patient is brought to the operating room with a right-sided peripheral vertigo. The provider makes a postauricular incision and uses an operating microscope to perform a mastoidectomy using a burr. He next destroys the semicircular canals, the utricle, and saccule completely removing the diseased labyrinth structures. The provider sutures the incision.
What CPT® code and ICD-10-CM codes are reported?
A physician sees a patient for the first observation visit, spends 85 minutes, with moderate MDM.
What CPT® code is reported?
Day 1 - A provider admits the patient to observation care for type 2 diabetes mellitus with hyperglycemia. The provider orders a HbA1c, a urine (microalbumin), and kidney function lab tests.
Blood sugar is high and poorly controlled. The provider discusses the case with the patient ' s endocrinologist. The provider prescribes an IV insulin drip, along with SQ insulin and keeps the
patient in observation overnight.
Day 2 - Patient is in observation care and the provider orders a blood glucose test. The patient ' s glucose levels have improved. The provider places an order for the dietitian to see the patient.
Provider
documents spending a total time of 25 minutes with the patient.
Day 3 - Patient has a blood glucose test. The patient ' s glucose level is back to normal. The provider documents spending 15 minutes with the patient. The provider discharges the patient.
What E/M coding is reported by the physician for the patient in observation care?
An 87-year-old male with a history of atrioventricular block and prior dual-chamber pacemaker implantation presents to the cardiology clinic for an in-person device evaluation. The physician performs a full electronic analysis of the pacemaker system, assessing atrial and ventricular lead function, battery status, sensing thresholds, and pacing thresholds. After the assessment, the pacemaker settings are adjusted to optimize heart rate response. The patient tolerates the procedure well and is advised to return for routine follow-up.
What CPT® code is reported?
(Regarding the CPT® Surgery Guidelines for a surgical code designated as a“Separate Procedure,”which statement isFALSE?)
A 4-week-old premature infant receives a 100 mg IM injection of RSV monoclonal antibody.
What CPT® codes are reported?
56-year-old female is postmenopausal with abnormal vaginal bleeding. Ob-gyn provider performs a hysteroscopy to examine the uterine cavity.
What CPT® code is reported?
An 8-year-old patient is placed under general anesthesia for treatment of a right orbital fracture due to a traumatic fall to the nose and face from a swing set. An on-call otolaryngologist is
asked to perform a general otolaryngologic examination to evaluate the patient. A mild nasal fracture is the diagnosis given by the otolaryngologist.
What is the CPT® and ICD-10-CM coding for the otolaryngologist ' s services?
A 23-year-old receives MMR and Hepatitis B vaccines without counseling.
What CPT® codes are reported?
(When a provider’s documentation refers touse, abuse, and dependenceof the same substance (e.g., alcohol), which statement is correct?)
What is the medical term for a procedure that creates a connection between the gallbladder and the small intestine?
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What CPT® and ICD-10-CM codes are reported?
(Dr. Winston sees a patient with abdominal pain in the observation unit in the hospital. This is hisfirst visitwith this patient during this stay. He spent a total time of85 minuteson that patient on that date of service, including review of the observation admission, labs, X-rays, and EKG results, and examining the patient with amoderate level of medical decision making. What CPT® coding is reported?)
A patient is diagnosed with compression fractures of the C6, C7 and T1 vertebrae. The patient agrees to have vertebroplasty. Bone cement is injected in the vertebral space until each of the two whole vertebral body is filled. The procedure is performed bilaterally.
What CPT® coding is reported?
A patient is diagnosed with sepsis due to enterococcus. What ICD-10-CM code is reported?
A 45-year-old has a dislocated patella in the left knee after a car accident. She taken to the hospital by EMS for surgical treatment. In the surgery suite, the patient is placed under general anesthesia. After being prepped and draped, the surgeon makes an incision above the knee joint in front of the patella. Dissection is carried through soft tissue and reaching the patella in attempt to reduce the dislocation. When the patella is exposed, it is severely damaged due to cartilage breakdown. The tendon is dissected and using a saw the entire patella is freed and removed. The tendon sheath is closed with sutures.
What procedure code is reported for this surgery?
View MR 005398
MR 005398
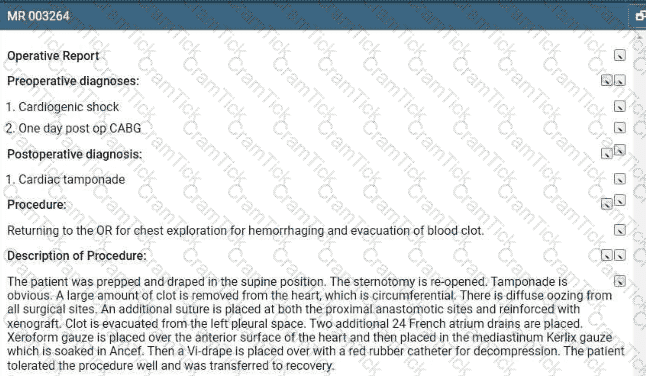
Operative Report
Preoperative Diagnosis: Nonfunctioning right kidney with ureteral stricture.
Postoperative Diagnosis: Nonfunctioning right kidney with ureteral stricture.
Procedure: Right nephrectomy with partial ureterectomy.
Findings and Procedure: Under satisfactory general anesthesia, the patient was placed in the right flank position. Right flank and abdomen were prepared and draped out of the sterile field. Skin incision was made between the 11th and 12th ribs laterally. The incision was carried down through the underlying subcutaneous tissues, muscles, and fascia. The right retroperitoneal space was entered. Using blunt and sharp dissection, the right kidney was freed circumferentially. The right artery, vein, and ureter were identified. The ureter was dissected downward where it is completely obstructed in its distal extent. The ureter was clipped and divided distally. The right renal artery was then isolated and divided between 0 silk suture ligatures. The right renal vein was also ligated with suture ligatures and 0 silk ties. The right kidney and ureter were then submitted for pathologic evaluation. The operative field was inspected, and there was no residual bleeding noted, and then it was carefully irrigated with sterile water. Wound closure was then undertaken using 0 Vicryl for the fascial layers, 0 Vicryl for the muscular layers, 2-0 chromic for subcutaneous tissue, and clips for the skin. A Penrose drain was brought out through the dependent aspect of the incision. The patient lost minimal blood and tolerated the procedure well.
What CPT® coding is reported for this case?
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What is the radiology coding for this encounter?
Which one of the following activities, when performed, is NOT considered when selecting an E/M service level based on time?
A 7-year-old boy was brought 10 the ED by his mother after he had been playing with small beads and one got lodged in his right external ear canal. After examination, the physician decided to remove the foreign body from the external auditory canal using alligator forceps without anesthesia.
What CPT® code is reported?
A 10-year-old had a cochlear implant in his left ear few weeks ago. Today he sees the audiologist to initialize and program the implant.
What CPT® code is reported?
A 47-year-old male with a history of peripheral artery disease presents with worsening claudication of the left leg. A diagnostic angiography confirms stenosis in the left iliac artery. To restore blood flow to the left leg, the vascular surgeon plans to perform angioplasty, using a balloon to dilate the vessel lumen followed by placement of an expandable stent in the left iliac artery.
What CPT® coding is reported for the procedure?
A suppression study includes five glucose tests and five growth hormone tests.
What CPT® coding is reported?
A patient who was experiencing severe abdominal pain underwent abdominal imaging and results showed several peritoneal tumors of various sizes.
The patient elected to have the tumors removed. An incision was made to access the intra-abdominal peritoneal cavity, where four tumors were identified, measured, and excised.
The largest was 2 cm, two were 1 cm each, and the smallest was 0.5 cm. Pathology report indicated the tumors were malignant.
What CPT® and ICD-10-CM coding is reported7
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What CPT® and ICD-10-CM code is reported?
Refer to the supplemental information when answering this question:
View MR 874276
What E/M code is reported?
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What CPT® and ICD-10-CM codes are reported?
(A patient is seen for nausea, vomiting, and sharp right lower abdominal pain. CT and labs support a diagnosis ofchronic appendicitis. The physician schedules anopen appendectomyand removes the appendix. What CPT® and diagnosis codes are reported?)
Which statement is TRUE for an Excludes2 note that is under a code in the Tabular List for ICD-10-CM?
(A wheelchair-bound resident of a skilled nursing facility is seen in the physician’s office. The physician’s office makes arrangements with a social worker to take the patient back to the skilled nursing facility. What is the HCPCS Level II transportation service code?)
(A patient has nausea with several episodes of emesis and severe stomach pain due to dehydration. Normal saline is infused in the same bag with2 mg ondansetron. Then15 mg ketorolac tromethamineis given for stomach pain. What J codes are reported for these services?)
Dr. Carter sees Mrs. White at the Spring Valley Nursing Facility. He saw her last month after she was admitted to the facility. Today is a follow up visit. She is doing well. He documented a medically appropriate history and exam. The patient has osteoporosis, hypertension, dementia. CAD, CHF, and type 2 diabetes (moderate number and complexity of problems). He reviews 4 labs and a telemetry (Moderate data). He adds a Cardizem prescription for better control of her blood pressure which is a moderate risk. What CPT® code does Dr. Carter report for the visit?
A 57-year-old woman with a physical status of 3 received general endotracheal anesthesia for a panniculectomy. The anesthesiologist personally performed the entire anesthesia service.
What CPT@ coding is reported for the anesthesia?
A patient who has HIV disease presents with loin pain in the clinic today. The patient reports he is having trouble sleeping due to the pain. What ICD-10-CM coding is reported?
(A trauma patient needs the following imaging:2 views nasal bones,3 views chest,2 views left forearm,2 views tibia/fibula. To exclude stroke, aCTA head with contrastis also ordered. What CPT® coding is reported?)
Which HCPCS Level II codes identify temporary services that would not be assigned a CPT® code, but are needed for claims processing purposes?
A patient presents to the urgent care facility with multiple burns acquired while burning debris in his backyard. After examination the physician determines the patient has third-degree burns of the left and right posterior thighs (10%). He also has second-degree burns of the anterior portion of the right side of his chest wall (8%) and upper back (6%). TBSA is 24% with third-degree burns totaling 10%.
What ICD-10-CM codes are reported, according to 1CD-10-CM coding guidelines?
A couple presents to the freestanding fertility clinic to start in vitro fertilization. Under radiologic guidance, an aspiration needle is inserted (by aid of a superimposed guiding-line) puncturing the ovary and preovulatory follicle and withdrawing fluid from the follicle containing the egg.
What is the correct CPT® code for this procedure?
(An orthopedic surgeon evaluated a patient in the emergency room two months after a surgical repair of a right radius and ulnar shaft fracture. After reinjury, imaging shows a displaced proximal fixation screw andmalunion of only the radial shaft. The same surgeon performs surgery to repair the malunion using a graft from the hip. What CPT® and diagnosis codes are reported?)
A patient with a history of a right-hand mass presents for outpatient surgical excision. The surgeon excises the 1.5 cm mass with margins using a scalpel with dissection extending through the dermis into the subcutaneous tissue. Hemostasis is achieved with electrocautery, and the wound is closed. Final pathology confirms the mass is a subcutaneous arteriovenous hemangioma.
Which CPT® and ICD-10-CM codes are reported?
(A 32-year-old visited a provider due to ongoing irritation and watering in his left eye. Suspecting an allergy, the provider carried out a test, introducing an allergenic extract into the mucous membrane inner lining of the eye. The patient’s eye is monitored for signs of an allergic reaction, such as redness and itching. What CPT® code is reported?)
A patient presents to the emergency room with a nosebleed that is controlled by limited anterior nasal packing.
What CPT® code is reported?
A patient presents with recurrent spontaneous episodes of dizziness of unclear etiology. Caloric vestibular testing is performed irrigating both ears with warm and cold water while evaluating the patient’s eye movements. There is a total of three irrigations.
What CPT® coding is reported?
The procedure is performed at an outpatient radiology department. From a left femoral access, the catheter is placed in the abdominal aorta and is then selectively placed in the celiac trunk and manipulated up into the common hepatic artery for an abdominal angiography. Dye is injected, and imaging is obtained. The provider performs the supervision and interpretation.
What CPT® codes are reported?
(Preoperative diagnoses:Bradycardia.
Postoperative diagnosis:Bradycardia.
Procedure performed:Dual-chamber pacemaker implantation.
Brief history:77-year-old female with recurrent syncope; evaluation revealed first-degree AV block, sinus bradycardia, bundle-branch block; bradyarrhythmia suspected; after discussion with her sister, dual-chamber pacemaker recommended; risks explained; consent obtained.
Procedure details:Taken to cardiac catheterization lab; positioned on cath table; prepped/draped standard; procedure challenging due to agitation despite adequate sedation; left infraclavicular area anesthetized with 0.5 cc Xylocaine; pacemaker pocket created; hemostasis with cautery; 9-French peel-away sheath used to introduce an atrial and a ventricular lead; leads positioned with excellent thresholds; secured with O-silk sutures over sleeves; pulse generator connected; pocket flushed with antibiotic solution; pacemaker/leads placed in pocket; incision closed in two layers; performed under fluoroscopic guidance.
Complication:None.
Plan:Return to recovery; discharge later this evening to nursing home with routine post-pacemaker care.
Question:What CPT® coding is reported for this procedure?)
View MR 001394
MR 001394
Operative Report
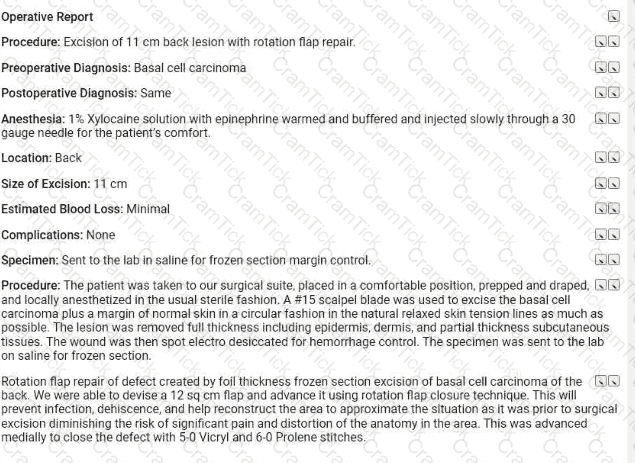
Procedure: Excision of 11 cm back lesion with rotation flap repair.
Preoperative Diagnosis: Basal cell carcinoma
Postoperative Diagnosis: Same
Anesthesia: 1% Xylocaine solution with epinephrine warmed and buffered and injected slowly through a 30-gauge needle for the patient ' s comfort.
Location: Back
Size of Excision: 11 cm
Estimated Blood Loss: Minimal
Complications: None
Specimen: Sent to the lab in saline for frozen section margin control.
Procedure: The patient was taken to our surgical suite, placed in a comfortable position, prepped and draped, and locally anesthetized in the usual sterile fashion. A #15 scalpel blade was used to excise the basal cell carcinoma plus a margin of normal skin in a circular fashion in the natural relaxed skin tension lines as much as possible The lesion was removed full thickness including epidermis, dermis, and partial thickness subcutaneous tissues. The wound was then spot electro desiccated for hemorrhage control. The specimen was sent to the lab on saline for frozen section.
Rotation flap repair of defect created by foil thickness frozen section excision of basal cell carcinoma of the back. We were able to devise a 12 sq cm flap and advance it using rotation flap closure technique. This will prevent infection, dehiscence, and help reconstruct the area to approximate the situation as it was prior to surgical excision diminishing the risk of significant pain and distortion of the anatomy in the area. This was advanced medially to close the defect with 5 0 Vicryl and 6-0 Prolene stitches.
What CPT® coding is reported for this case?
(A patient is diagnosed with agangrenous ulceron theright thighwith thefat layer exposedand is currently being treated. What ICD-10-CM coding is reported?)
A 67-year-old patient has osteomyelitis of the shoulder blade and is in surgery to remove the sequestered section of dead infected fragment bone from surrounding bone.
What CPT® code is reported?
(A patient presents with dysuria and lower abdominal pain. The physician suspects UTI. Anautomated urinalysis without microscopyis done in the office and isnegative. UTI is ruled out for the final diagnosis. What CPT® and ICD-10-CM codes are reported?)
(A 40-year-old woman with progressive sensorineural hearing loss in the right ear has acochlear implantplaced for the right ear. Anesthesia is provided by aCRNAwithmedical directionby an anesthesiologist who is concurrently directing 5 CRNAs. Physical status is3. What anesthesia CPT® and ICD-10-CM codes are reported by theanesthesiologist?)
A patient undergoes a percutaneous liver biopsy with ultrasound guidance for primary biliary cirrhosis.
What CPT® and ICD-10-CM codes are reported?
A patient presents to the office with dysuria and lower abdominal pain. The physician suspects she has a UTI. A non-automated urinalysis is done in the office and is negative. UTI is ruled out
for the final diagnosis.
What CPT and ICD-10-CM codes are reported?
A patient with Parkinson ' s has sialorrhea. The physician administers an injection of atropine bilaterally into a total of four submandibular salivary glands.
What CPT® coding is reported?
Refer to the supplemental information when answering this question:
View MR 003264
What is the procedural coding?
Refer to the supplemental information when answering this question:
View MR 903096
What CPT® and ICD-10-CM coding is reported?
(Which punctuation is used in the ICD-10-CM Tabular List to denotesynonyms, alternative wording, or explanatory phrases?)
Refer to the supplemental information when answering this question:
View MR 623654
What CPTO coding is reported for this case?
A patient with three thyroid nodules is seen for an FNA biopsy. Using ultrasonic guidance, the provider inserts a 25-gauge needle into each nodule. Nodular tissue is aspirated and sent to pathology.
What CPT® coding reported?
A patient undergoes angioplasty with stent placement in the left iliac artery.
What CPT® coding is reported?
A cardiologist uses the hospital ' s equipment for a cardiac stress test as he doesn ' t own equipment for the test. He supervises the test and provides the interpretation and report of the test.
What CPT® codes are reported?
(A 58-year-old patient undergoes diagnostic facet joint injections. The physician performsbilateral paravertebral facet joint injectionsat theT2–T3, T3–T4, and T4–T5levels, usingfluoroscopic guidanceat each site. What CPT® coding is reported for this encounter?)
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
Which CPT® and ICD-10-CM codes are reported for this procedure?
A patient suffering from idiopathic dystonia is seen today and receives the following Botulinum injections: three muscle injections in both upper extremities and seven injections in six paraspinal muscles.
How are these injections reported according to the CPT® guidelines?
What does the term “manipulation” refer to in the context of fracture or dislocation treatment?
A 42-year-old male is diagnosed with a left renal mass. An abdominal incision along with rib resection is made to expose and access the kidney. The left kidney is removed, along with surrounding fat, adrenal gland, lymph nodes in the area, and the incision site is sutured. What CPT ® code is reported for this procedure?
(What CPT® coding is reported for the insertion ofHeyman capsulesfor clinical brachytherapy?)
A patient with lateral epicondylitis of the left elbow is taken to the operating room for manipulation under general anesthesia. The physician performs stretching and rotation to restore motion.
What CPT® coding is reported for the physician?
A patient presents to the labor and delivery department for a planned cesarean section for triplets. She is at 37 weeks gestation. She is given a continuous epidural for the delivery.
What anesthesia coding is reported?
A 25-year-old woman underwent percutaneous breast biopsy on the right breast with placement of a Gelmark clip. The procedure was performed using stereotactic imaging.
What CPT® codes will be reported?
(A patient training for a marathon collapsed due to heat exhaustion on a very hot day and is treated at a nonfacility urgent care center. The physician diagnoses heat exhaustion and dehydration and begins IV therapy of normal saline (pre-packaged fluid and electrolytes). The hydration lasts1 hour and 30 minutes. What CPT® coding is reported?)
The CPT® code book provides full descriptions of medical procedures, with some descriptions requiring the use of a semicolon (;) to distinguish among closely related procedures.
What is the full description of CPT® code 35860?
A 55-year-old female patient is diagnosed with renal cell carcinoma. She is having a resection of the affected kidney, a portion of the ureter, and rib resection, open aproach. The procedure is complicated due to a prior surgical procedure performed on the same kidney.
What CPT® coding is reported?
A 35-year-old female has cancer in her left breast. The surgeon performs a mastectomy, removing the breast tissue, skin, pectoral muscles, and surrounding tissue, including the axillary and internal mammary lymph nodes.
Which mastectomy code is reported?
A physician performs excisional debridement on multiple wounds:
Lower back: 12 cm, involving fascia
Left shoulder: 8 cm, involving subcutaneous tissue
Left lower leg: 16 cm, involving subcutaneous tissue
What CPT® codes are reported?
A patient is sent to the hospital by his family care provider for admission due to a high fever and neck pain The patient is admitted to the hospital to rule out bacterial meningitis. The hospitalist admits the patient and orders a CBC. CMR Blood culture, CT of the head and chest, and a lumbar puncture (spinal tap). After review of the results, he determines the patient has bacterial meningitis and starts the patient on IV antibiotics.
What CPT® and ICD-10-CM codes are reported for the admission?
(A 28-year-old woman who is 36 weeks pregnant withdichorionic/diamniotic twinsdeliveredboth babies vaginally. The same OB provider who delivered the babies provided theantepartum careand will provide thepostpartum care. What CPT® and ICD-10-CM codes are reported on the maternal record?)
Which place of service code is submitted on the claim for a service that is performed in a skilled nursing facility?
A patient with compression fractures of L5 and the sacrum undergoes vertebroplasty, with cement injected into two vertebral bodies, performed bilaterally.
What CPT® coding is reported?
The patient, who is at 32 weeks pregnant, has been hospitalized due to an infection of COVID-19.
What ICD-10-CM codes are reported?
A 50-year-old patient presented with a persistent cough has not responded to standard treatments. The patient ' s physician decides to perform a flexible bronchoscopy with bronchial biopsies to further investigate the cause. A flexible bronchoscope is inserted through the patient ' s mouth and into the bronchial tubes. Five biopsies are taken for further testing. The biopsies were sent to the lab for analysis to determine the next steps in the patient ' s treatment plan.
What CPT® coding is reported?
An 8-year-old undergoes tonsillectomy with adenoidectomy for chronic tonsillitis and adenoiditis with hypertrophy.
What CPT® and ICD-10-CM codes are reported?
Four malignant peritoneal tumors are excised, the largest measuring 15 cm.
What CPT® and ICD-10-CM coding is reported?
Patient has esotropia of the right eye and presents to operating suite for strabismus surgery. The physician resects the medial rectus horizontal and lateral rectus muscles of the eye and secures them with adjustable sutures. Extensive scar tissue is noted, due to a previous surgery involving an extraocular muscle. Extraocular muscle is isolated, and the muscle is freed from surrounding scar tissues.
What CPT® codes are reported for this surgery?
A patient is diagnosed with diabetic polyneuropathy.
Using ICD-10-CM coding guidelines, what ICD-10-CM coding is reported?
A 26-year-old male presents with a deep laceration from a kitchen knife to his right hand. The surgeon washes the open wound with sterile saline. Clamps are applied. The provider cleans the
vessel and prepares the edges of thee wound. She then repairs the bleeding vessel with sutures. The clamps are removed and the provider uses a Doppler probe to check the blood flow pattern
through the repaired vessel.
What CPT® code is reported?
A patient is taken to the radiology department for a radiological cardiac catheterization. An acute MI of the left anterior descending coronary artery is found. The cardiologist performs a suction thrombectomy, followed by atherectomy and a stent to the artery. A CRNA provides MAC for this patient, who is status P5.
What code/modifier combination would you report for the services of the CRNA?
A 44-year-old female patient came in for a planned laparoscopic total abdominal hysterectomy for endometriosis of the uterus. The surgeon attached the trocars, a scope is inserted examining
the uterus, abdominal wall, bilateral ovaries, and fallopian tubes. The surgeon decided to convert the laparoscopic procedure to an open total hysterectomy because of the extensive amount of
adhesions that need to be removed. A total hysterectomy was performed and due to removal of the extensive adhesions the surgery took longer than normal of 2 hours.
What CPT® and diagnosis codes are reported?
This 27-year-old male has morbid obesity with a BMI of 45 due to a high calorie diet. He has decided to have an open Roux-en-Y gastric bypass. The patient is brought to the operating room and placed in supine position. A midline abdominal incision is made. The stomach is mobilized, and the proximal stomach is divided and stapled creating a small proximal pouch in continuity with the esophagus. A short limb of the proximal bowel of 155 cm is divided. It is brought up and anastomosed to the gastric pouch. The other end of the divided bowel is connected back into the distal small bowel to the short limb ' s gastric anastomosis to restore intestinal continuity. The abdominal incision is closed.
What are the procedure and diagnosis codes for this encounter?
An air bag deployed when a driver lost control of the car and crashed into a guardrail on the side of the highway. The driver suffers partial impact resulting in a skull fracture of the anterior
cranial base. The fracture is diagnosed using the MRI scanner and cerebrospinal fluid is noted dripping via the sphenoid sinus into the right nasal passage. The patient requires a surgical nasal
sinus endoscopy to assess and repair the injury.
What is the correct procedure and diagnosis coding combination to report this service?
A patient is seen at the doctor ' s office for nausea, vomiting, and sharp right lower abdominal pain. CT scan of the abdomen is ordered. Labs come back indicating an increased WBC count with
review of the abdominal CT scan. The physician determines the patient has chronic appendicitis. The physician schedules an appendectomy and takes the patient to the operating room. The
appendix is severed from the intestines and removed via scope inserted through an umbilical incision. What CPT® and diagnosis codes are reported?
A male patient passes out while jogging in the park. Upon examination at the hospital, he is found to have a wide complex tachycardia and undergoes an electrophysiologic study and radiofrequency ablation. For this procedure he is placed under general anesthesia.
What is the anesthesia coding for this otherwise healthy 35-year-old?
A 49-year-old patient arrives with hearing loss in his left ear. Impedance testing via tympanometry is performed.
What CPT® code is reported?
(A patient presents for surgery due to recurrent lumbar radiculopathy at a previously operated spinal level. The surgeon performs arepeat exploration laminotomywithbilateral foraminotomyto decompress nerve roots at theL1–L2 interspace. No additional spinal levels are treated. What CPT® coding is reported?)
(A female patient underwent a mastectomy on herleft breastlast year due to breast cancer. The surgery was successful in eliminating the cancer and no further treatment was required. However, a recent diagnosis now includes cancer thatmetastasized to her liver. What ICD-10-CM coding is reported?)
A patient complains of tarry, black stool, and epigastric tightness. An esophagogastroduodenoscopy is recommended to evaluate the source of the bleeding. The endoscope is inserted orally. The esophagus appears normal on scope insertion. No evidence of bleeding in the stomach. The scope is then passed into the duodenum, where a polyp is found and removed with hot biopsy forceps. No evidence of bleeding post procedure.
What CPT® code is reported?
A driver loses control of a vehicle and crashes into a guardrail on the side of the highway. The patient sustains a fracture of the anterior fossa cranial base. Imaging confirms Involvement of the sphenoid sinus, but no cerebrospinal fluid (CSF) leak is identified. The patient undergoes a surgical nasal sinus endoscopy with sphenoidotomy lo evaluate and treat the sinus injury. No CSF leak repair is performed.
What is the correct procedure and diagnosis coding combination to report this service?
(A 65-year-old male patient passed away due to unknown causes. An autopsy was ordered by the attending physician to determine the cause of death. The pathologist performed agross and microscopic examination autopsy, that includes thebrain and spinal cord. What CPT® coding is reported?)
Which statement is NOT true regarding the ICD-10-CM coding guidelines for burns?
A 52-year-old woman has been experiencing discomfort and itching In the vulvar area for several months. She has a history of abnormal Pap smears and a recent biopsy revealed vulvar intraepithelial neoplasia (VIN III). Decision has been made to perform a vulvectomy.
Procedure: Under general anesthesia, the surgeon made an incision in the vulvar area and removed the vulva (more than 80%), including the affected skin and deep subcutaneous tissue.
What CPT® and ICD-10-CM codes are reported?
An otolaryngologist removes a 3 cm deep facial tumor within muscle.
What CPT® code is reported?
A patient who is 37 weeks ' gestation is admitted to labor and delivery for a cesarean delivery. An external cephalic version was performed successfully several days ago and she now presents in labor, fully dilated, and the fetus has returned to a footling presentation.
What anesthesia code is reported?
Eric is buying his first life insurance policy from XYZ Life Insurance Company. The company requires Eric have a physical exam prior to issuance of the policy. Eric sees his primary care provider who completes the required documentation and forms provided by the insurance company.
How does the primary care provider report his services?
(What ICD-10-CM coding is reported forType 1 diabeteswithdiabetic chronic kidney disease?)
A patient has chronic cholesteatoma in the right middle ear. The otolaryngologist performed a tympanoplasty with a radical mastoidectomy, removing the middle ear cholesteatoma. Grafting
technique was used to repair the eardrum with ossicular chain reconstruction.
What CPT® code is reported for this surgery?
A 64-year-old with congestive heart failure (CHF) has pericardial effusion. The provider inserts a needle under ultrasound guidance, aspirating the fluid from the pericardial sac.
What CPT® coding is reported?
A complete 7-view X-ray of the lumbosacral spine, including bending views, is performed.
What CPT® code is reported?
A physician prescribes carbamazepine to treat a patient with epileptic seizures. After six months, the physician performs a therapeutic drug test to monitor the total level of the drug in the patient.
What CPT® and ICD-10-CM coding is used for the six month-evaluation?



TESTED 06 Jul 2026